![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
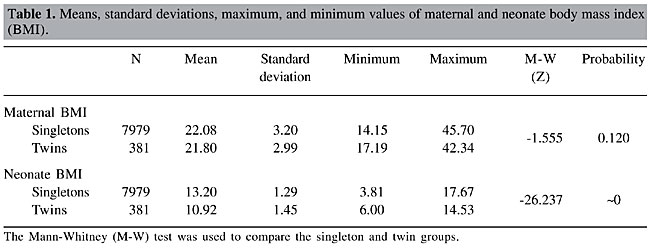
ABSTRACT. We examined the correlation between maternal prepregnancy body mass index (BMI) and newborn weight, length, BMI, and gestational order, in singleton and twin births. The sample comprised 381 mothers of multiple babies (562 twins), and 7979 singleton pregnancies, used as controls. The Mann-Whitney non-parametric test was used to compare the values between the two groups, and the Spearman’s correlation test (rS) was applied to the quantitative variables. A significant positive correlation was found with singleton baby variables: the higher the maternal BMI, the higher the newborn’s BMI, weight, length, and gestational order. However, no significant correlation was found between maternal BMI and any of these variables in twins. Maternal weight gain, in the twin group, showed a significant positive correlation with the newborn gestational order (rS = 0.154; P = 0.002), weight (rS= 0.493; P < 0.001), length (rS = 0.469; P < 0.001), and BMI (rS = 0.418; P < 0.001). In singletons, the correlation was positive with all the variables, except for the gestational order. The newborn BMI was significantly higher in twins born by C-section than those born by vaginal birth (Z = -4.974; P < 0.001). Mothers of singletons delivered by C-section had a significantly higher BMI than those of singletons born by vaginal birth (Z = -1.642; P < 0.001); however, no significant differences were observed in mothers of twins. Prepregnancy maternal BMI in twin births would not be predictive of newborns weight, length and BMI in this population. Maternal weight gain during pregnancy proved to be the most adequate for predicting the weight, length and BMI of twins delivered by C-section. Key words: Prepregnancy BMI, Gestational age, Maternal weight gain, Maternal obesity INTRODUCTION A woman’s nutritional condition has been considered as an important indicator of the perinatal result. There is a direct correlation between maternal nutritional condition and weight at birth, thus, the body mass index (BMI = weight/height2) has been used as an epidemiological factor predictive of fetal growth (Lizo et al., 1998; Merchant et al., 1999; Bolzan and Guimarey, 2001). A low prepregnancy BMI is one of the strongest predictors of adverse perinatal results, such as premature birth and fetal growth restrictions (Neggers and Goldenberg, 2003). Newborns to mothers with a BMI one standard deviation below average were smaller, and their relative risk of presenting intrauterine growth restriction was twice as high (Bolzan and Guimarey, 2001). An impaired maternal nutritional condition, as indicated by low weight, height and BMI, is associated with small babies, with smaller cephalic perimeters (Thame et al., 1997). On the other hand, the BMI increased with advanced maternal age, higher parity and increased gestational age (Wolfe et al., 1991). Risks of developing maternal obesity, gestational diabetes, preeclampsia, fetal macrosomia, and shoulder dystocia are comparatively predictable, either by maternal weight or by BMI (Wolfe et al., 1991). In the long run, both maternal weight and BMI explain the association between weight at birth and BMI at an adult age (Parsons et al., 2001). On the other hand, the factors that affect both birthweight and adult BMI are partly genetic and partly non-shared environmental (Whitfield et al., 2001). Generally, the BMI estimates of heritability show values between 0.24 and 0.40, when derived from family data, and 0.70 when derived from twin data (Schousboe et al., 2003). According to Allison et al., 2003, this happens when non-additive effects (gene-gene or gene-environment interactions) are important, which most likely is the case for BMI. Prepregnancy BMI in the gestation of multiple fetuses has been studied, particularly to determine the ideal maternal weight gain and weight of twin newborns, to allow for specific recommendations to this population (Lantz et al., 1996), or even to analyze its usefulness in predicting maternal diseases (Jensen et al., 2003). Our objective was to determine if there was an association between maternal prepregnancy BMI and some anthropometric characteristics of the newborn, these being, weight, height and BMI, in single and twin gestations, in a high-socioeconomic level population. MATERIAL AND METHODS Prepregnancy BMI (weight/height2) was calculated in 381 mothers of multiple babies and was compared to the weight at birth, length and BMI of their respective twin babies (562 newborns) in a high-socioeconomic level population, classified according to the degree of education (Zurayk et al., 1987; Alonso et al., 1997). This study used data retrospectively collected from the obstetric records of twin gestations and the respective newborns, from 1990-1999. The control group included 7979 singleton gestations that occurred in the same study period. The data on maternal prepregnancy weight were obtained from the mother, and the newborn’s weight was recorded immediately after birth. The newborn’s length was measured with an anthropometric ruler, at the Neonatal Unit, between 6 and 12 h after birth, according to the standards in place at the institution. The data were collected from medical records, so it was not necessary to obtain informed consent. The statistical analyses performed were the following non-parametric tests: Mann-Whitney test (Z) for every comparison between two groups, the Kruskal-Wallis test (c2) to compare more than two groups, and the Spearman correlation test (rS) for the quantitative variables: BMI, weight, length, and gestational order. The software used was SPSS,V11.5 (Statistical Package for Social Sciences). RESULTS A comparison was made of BMI values between the singletons and twins (Table 1). There was no significant difference between the BMI of mothers of singletons and twins (P = 0.12); however, the singletons’ BMI was significantly higher than that of twins (P < 0.001), as would be expected.
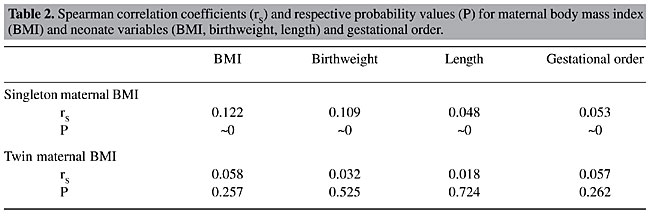
Spearman’s correlation coefficients between maternal BMI and the variables, newborn BMI, weight, length, and the gestational order were calculated (Table 2). There was a significant positive correlation with all variables in singletons, that is, the higher the maternal BMI, the higher the newborn’s BMI, as well as the higher the weight, length and gestational order. However, there was no correlation between maternal BMI and any of these variables in twins, that is, the twins’ BMI, weight and length did not depend on maternal BMI. Likewise, the gestational order, in the case of the twins, also did not prove to be correlated with the maternal BMI.
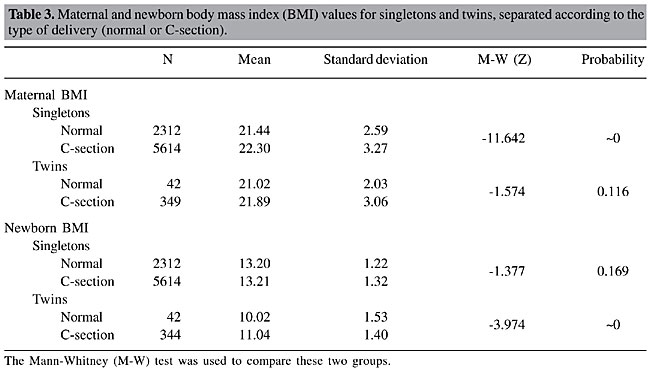
We examined these correlations at different gestational ages, which are normally lower in twins. Up to and including the 36th week of pregnancy, there was no significant correlation in both single and twin births. However, when the 37th week of pregnancy was included in the analysis, a significant correlation was observed between maternal BMI and that of the newborn (rS = 0.073; P = 0.017) only in singletons. We then focused on the correlation between maternal weight gain and the following variables: prepregnancy maternal BMI, gestational order, and the newborn’s weight, length and BMI. There was a negative correlation in singletons (rS = -0.033; P = 0.003) with the gestational order and a positive correlation with the newborn’s weight (rS = 0.230; P < 0.001), length (rS = 0.165; P < 0.001) and BMI (rS = 0.212; P < 0.001). In the twin group, there was a significant positive correlation with all these variables: gestational order (rS = 0.154; P = 0.002), weight (rS = 0.493; P < 0.001), length (rS = 0.469; P < 0.001), and BMI of the newborn (rS = 0.418; P < 0.001). On the other hand, the average maternal weight gain was higher in women who had cesarean deliveries (C-sections), both for singletons and twins. In order to study the association between prepregnancy maternal BMI and the type of delivery (vaginal or C-section), the means were calculated and the Mann-Whitney test was used on maternal and newborn’s BMI values, comparing between singleton and twin births. Mothers of singletons born by C-section had a significantly higher BMI than the mothers of singletons born by vaginal birth (Z = -1.642; P < 0.001; Table 3). However, the BMI of mothers of twins was not significantly different between those who had vaginal deliveries versus C-sections. On the other hand, when the newborn’s BMI was examined, it was noted that, in the case of singletons, there was no difference in the BMI of babies born by vaginal birth or C-section, but in the case of twins, a significantly higher BMI was observed in babies born by C-section (Z = -3.974; P < 0.001).
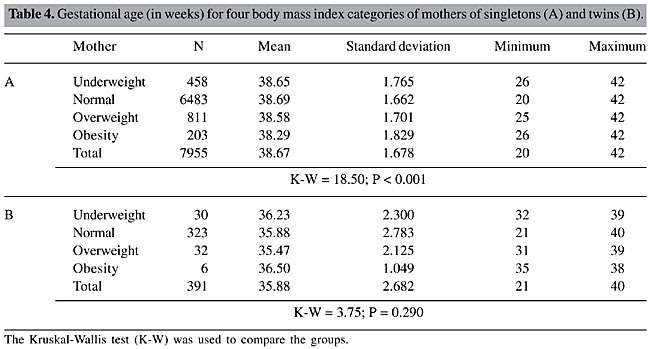
Since the weight reflects the gestational age, these newborn gestational ages were initially analyzed according to the type of delivery. It was found that in singletons the average gestational age for vaginal birth was 38 6/7 weeks, and in C-sections it was 38 4/7 weeks, a significant difference according to the Mann-Whitney test (Z = -6.469; P < 0.001). In twins, however, the situation was the opposite; the mean gestational age for twin babies born by vaginal birth was 34 weeks, significantly lower than that of those born by C-section, with a mean of 36 weeks (Z = -3.954; P < 0.001). Subsequently, the newborn gestational age was compared, using the Kruskal-Wallis test, for four groups of prepregnancy maternal BMI: low weight, normal weight, overweight, and obesity (Table 4A); there were significant differences (c2 = 18.50; P < 0.001). Obese mothers had babies with a significantly lower gestational age than that of the other three groups, which did not differ significantly from each other. In the case of mothers of twins, there was no significant difference between the four groups for gestational age (c2 = 3.75; P = 0.290; Table 4B).
When the four BMI groups were compared, it was found that the proportion of mothers of singletons who underwent C-sections increased significantly with BMI classification, starting with 61.7% in the underweight group, 69.8% for normal weight, 80.9% for overweight, and 85.6% in the obese mothers (c2 = 82.90; P < 0.001). In mothers of twins, a similar result was also observed (80.0, 89.2, 86.9, and 100%), though the tendency was not significant, perhaps due to the small number of mothers classified as underweight or obese. DISCUSSION Maternal BMI has been used as an epidemiological factor predictive of fetal growth (Bolzan and Guimarey, 2001). On the other hand, the factors which affect both birthweight and adult BMI are partly genetic and partly non-shared environmental (Whitfield et al., 2001). We examined the correlation of prepregnancy maternal BMI with anthropometric characteristics of the newborn, in single and twin gestations, among mothers from a high-socioeconomic level population, based on their level of education (Zurayk et al., 1987; Alonso et al., 1997); all mothers had prenatal follow-up. We found pregnant women who were classified in all BMI classes. Prepregnancy maternal BMI showed a positive association with the newborn’s weight and length and the gestational order for singletons. This association was also noted by several other authors (Wolfe et al., 1991; Thame et al., 1997; Luke et al., 1997; Bolzan and Guimarey, 2001; Parsons et al., 2001; Jensen et al., 2003; Szklarska and Jankowska, 2003). However, in the twin gestations we examined, no association was found between prepregnancy maternal BMI and the variables newborn weight, length and gestational order, which differs from the conclusions of Luke et al. (1977). Luke et al., 2003, found that optimal rates of fetal growth and birth weights in twins are achieved at rates of maternal weight gain that vary by period of gestation and maternal prepregnancy BMI status. The optimal weight gain of twins corresponded to a gestational age equal to or greater than 36 weeks. Consequently, we tried to determine whether the gestational age could have an influence, since in twin gestations it was significantly lower than for single gestations. In fact, the behavior in single gestations was similar to that of twin gestations up to the 36th week, that is, no association was found. From the 37th week on, this association was present only in singletons. The fact that there was an average gestational age of twins of 36 weeks in our study, could explain the difference between the findings. On the other hand, Beiguelman et al., 1998, found that the pattern of twin fetal growth rate was delayed when compared to that of singletons, regardless of the socioeconomic level of the inpatients. They also found that the fetal growth rates of twins and singletons were similar up to about 28 weeks of gestation, and from this age on a slower twin intrauterine growth began; this difference then progressively increased. Recently, Colletto et al. (2004), in a study of three different socioeconomic level hospitals, found that up to 36th week of gestation, the birthweight of twins did not differ, and only from then on, the growth curve of the highest socioeconomic level hospital began to show a higher birth weight. Another factor studied was the type of delivery; it was found that, prepregnancy maternal BMI was higher for those mothers who underwent C-section in single gestations, which could be related to maternal obesity, since C-sections are more frequent in obese mothers (Loverro et al., 2001; Jensen et al., 2003). There was no significant difference in prepregnancy maternal BMI according to the type of delivery for twin gestations, since the indication for C-section would be related to the nature of the twin gestation itself, and not to a specific maternal condition, that is, obesity. For single gestations, maternal weight gain up to delivery was significantly higher in C-sections than in vaginal births. Moreover, a positive association was found with the newborn’s birthweight and length, only for vaginal birth (higher than that in C-sections), but not with the newborn’s BMI. The gestational age also varied significantly according to the type of delivery; it was higher for vaginal birth than for C-sections. In twin gestations, maternal weight gain was significantly higher in C-sections than in vaginal births, showing a positive association of this type of delivery with the newborn’s weight, length and BMI. Kanadys and Oleszczuk (2000) found that vaginal birth is associated with smaller maternal weight gain rates in twin births. Another explanation for this fact could be the finding of a significant difference in gestational age, which was higher in twins born by C-section, close to term, compared to frequent prematurity for twins born by vaginal birth. According to Riese et al., 2003, maternal weight gain is associated with the weight at birth of twins at term and of the female gender, but not for pre-term twins of the male gender. Finally, in the analysis of the newborn gestational age according to the four groups of prepregnancy maternal BMI, that is, low weight, normal weight, overweight, and obesity, there were significant effects in the group of mothers of singletons. Obese mothers had babies with a significantly lower gestational age than mothers in the other three groups, indicating interventionist obstetric behavior involving obese mothers of singletons. However, in the case of twin gestations, no significant differences were observed. CONCLUSIONS In twin gestations, no association was found between prepregnancy maternal BMI and the variables newborn weight, length, BMI, and gestational order. There was no significant effect of prepregnancy maternal BMI on the type of birth in twin gestations; however, differences were found in the case of singletons. In twin gestations, maternal weight gain was significantly higher in C-sections than in vaginal deliveries, showing a positive association with the newborn’s weight, length and BMI for C-sections. Thus, prepregnancy maternal BMI in twin gestations cannot be considered as predictive of the newborn’s weight, length and BMI in this population. Maternal weight gain during pregnancy proved to be more adequate to predict the twins’ weight, length and BMI in the case of C-section delivery. REFERENCES Allison, D.B., Pietrobelli, A., Faith, M.S., Fontaine, K.R., Gropp, E. and Fernández, J. (2003). Genetic influences on obesity. In: Obesity (Eckel, R., ed). Elsevier, New York, NY, USA. Alonso, J., Perez, P., Saez, M. and Murillo, C. (1997). Validity of occupation as an indicator of social class according to the British Registar General Classification. Gac. Sanitaria 11: 205-213. Beiguelman, B., Colletto, G.M.D.D., Franchi-Pinto, C. and Krieger, H. (1998). Birth weight of twins: 1. The fetal growth patterns of twins and singletons. Gen. Mol. Biol. 21: 151-154. Bolzan, A.G. and Guimarey, L.M. (2001). Relationship between body mass index during pregnancy in adolescent and adult women, anthropometric indicators of fetal growth and intrauterine growth retardation. Arch. Latinoam. Nutr. 51: 145-150. Colletto, G.M.D.D., Segre, C.A.M. and Rielli, S.T.R.C. (2004). Influence of socioeconomic levels on birth weight of twins and singletons. Twin Res. 7: 128-133. Jensen, D.M., Damm, P., Sorensen, B., Molsted-Pedersen, L., Westergaard, J.G., Ovesen, P. and Beck-Nielsen, H. (2003). Pregnancy outcome and prepregnancy body mass index in 2459 glucose-tolerant Danish women. Am. J. Obstet. Gynecol. 189: 239-244. Kanadys, W.M. and Oleszczuk, J. (2000). Maternal weight gain during twin pregnancy. Its relationship to the incidence of preterm delivery. Ginekol. Pol. 71: 1355-1359. Lantz, M.E., Chez, R.A., Rodriguez, A. and Porter, K.B. (1996). Maternal weight gain patterns and birth weight outcome in twin gestation. Obstet. Gynecol. 87: 551-556. Lizo, C.L., Azevedo-Lizo, Z., Aronson, E. and Segre, C.A. (1998). Relationship between maternal weight gain and birthweight. J. Pediatr. 74: 114-118. Loverro, G., Greco, P., Vimercati, A., Nicolardi, V., Varcaccio-Garofalo, G. and Selvaggi, L. (2001). Maternal complications associated with cesarean section. J. Perinat. Med. 29: 322-326. Luke, B., Keith, L. and Keith, D. (1997). Maternal nutrition in twin gestations: weight gain, craving and aversions, and sources of nutrition advice. Acta Genet. Med. Gemellol. 46: 157-166. Luke, B., Hediger, M.L., Nugent, C., Newman, R.B., Mauldin, J.G., Witter, F.R. and O’Sullivan, M.J. (2003). Body mass index - specific weight gains associated with optimal birth weights in twin pregnancy. J. Reprod. Med. 5: 529-537. Merchant, S.S., Momin, I.A., Sewani, A.A. and Zuberi, N.F. (1999). Effect of pregnancy body mass index and gestational weight gain on birth weight. J. Pak. Med. Assoc. 49: 23-25. Neggers, Y. and Goldenberg, R.L. (2003). Some thoughts on body mass index, micronutrient intakes and pregnancy outcome. J. Nutr. 133: 1737s-1740s. Parsons, T.J., Power, C. and Manor, O. (2001). Fetal and early life growth and body mass index from birth to early adulthood in 1958 British cohort: longitudinal study. Br. Med. J. 323: 1331-1335. Riese, M.L., Swift, W.M. and Barnes, S.L. (2003). Newborn twin outcome predicted by maternal variables: differentiation by term and sex. Twin Res. 6: 12-18. Schousboe, K., Willemsen, G., Kyvik, K.O., Mortensen, J., Boomsma, D.I., Cornes, B.K., Davis, C.J., Fagnani, C., Hjelmborg, J., Kaprio, J., De Lange, M., Luciano, M., Martin, N.G., Pedersen, N., Pietilainen, K.H., Rissanen, A., Saarni, S., Sorensen, T.I., Van Baal, G.C. and Harris, J.R. (2003). Sex differences in heritability of BMI: a comparative study of results from twin studies in eight countries. Twin Res. 6: 409-421. Szklarska, A. and Jankowska, E.A. (2003). Independent effects of social position and parity on body mass index among Polish adult women. J. Biosoc. Sci. 35: 575-583. Thame, M., Wilks, R.J., McFarlane-Anderson, N., Bennet, F.I. and Forrester, T. (1997). Relationship between maternal nutritional status and infant’s weight and body proportions at birth. Eur. J. Clin. Nutr. 51: 134-138. Whitfield, J.B., Treloar, S.A., Zhu, G. and Martin, N.G. (2001). Genetic and non-genetic factors affecting birth-weight and adult body mass index. Twin Res. 4: 365-370. Wolfe, H.M., Zador, I.E., Gross, T.L., Martier, S.S. and Sokol, R.J. (1991). The clinical utility of maternal body mass index in pregnancy. Am. J. Obstet. Gynecol. 164: 1306-1310. Zurayk, H., Halabi, S. and Deeb, M. (1987). Measures of social class based on education for use in health studies in developing countries. J. Epidemiol. Community Health 42: 173-179. |
|